diabetes insipidus: Best 5 questions to ask your doctor

appointment can transform your diabetes insipidus management
journey.
Introduction: Are You Really Asking Your Doctor the Right Questions About Diabetes Insipidus?
Did you know that diabetes insipidus affects approximately 1 in 25,000 people worldwide, yet studies show that nearly 60% of newly diagnosed patients leave their first doctor’s appointment feeling confused and under-informed? If you or someone you love has recently been diagnosed with diabetes insipidus (DI), you are not alone — and more importantly, you are not powerless.
Unlike the far more commonly known diabetes mellitus (Type 1 or Type 2), diabetes insipidus is a rare but serious condition affecting the body’s ability to regulate fluid balance.
It has nothing to do with blood sugar. Instead, it involves the kidneys’ inability to properly conserve water, leading to excessive thirst (polydipsia) and the excretion of abnormally large volumes of dilute urine (polyuria).
Here is the hard truth: most patients don’t know what questions to ask their endocrinologist or nephrologist. That gap in communication can delay proper treatment, worsen symptoms, and significantly impact quality of life.
This blog post is your comprehensive, doctor-visit-ready guide. We have identified the 5 best questions to ask your doctor about diabetes insipidus, backed by clinical data and expert-level insights, so you can walk into that appointment empowered, informed, and ready to take control of your health journey.
💡 Pro Tip: Bookmark this page and bring it with you to your next appointment!
What Is Diabetes Insipidus? A Quick Medical Overview
have is the essential first step toward effective, personalized
treatment.
Before diving into the questions, let’s establish a clear clinical foundation so that every question you ask makes sense in context.
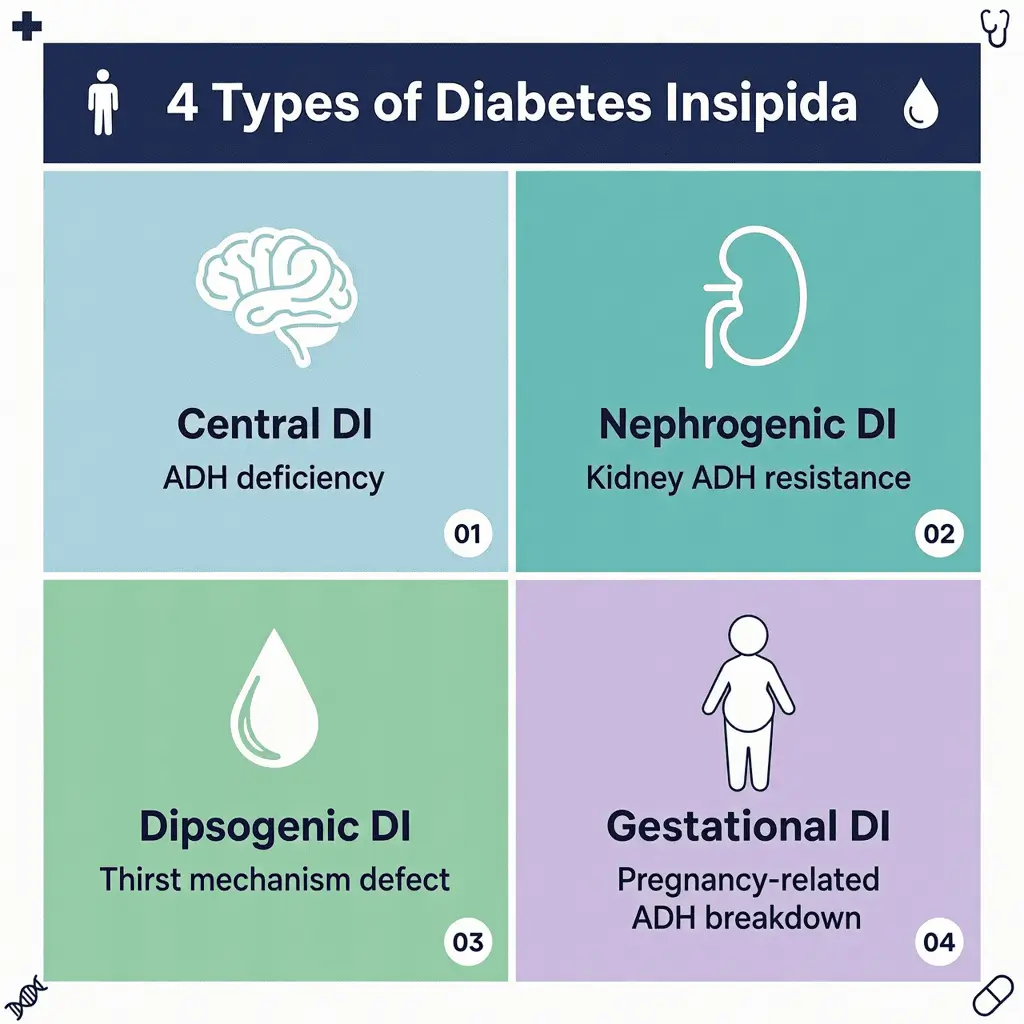
Diabetes insipidus is a disorder characterized by the disruption of the body’s fluid-regulating mechanism. There are four main types of diabetes insipidus:
| Type | Cause | Key Feature |
| Central DI | Deficiency of ADH (vasopressin) due to hypothalamus/pituitary damage | Most common type |
| Nephrogenic DI | Kidneys fail to respond to ADH | Often genetic or medication-induced |
| Dipsogenic DI | Defect in thirst mechanism | Excessive fluid intake |
| Gestational DI | Enzyme destroys ADH during pregnancy | Temporary, pregnancy-related |
Key NLP-related terms you will encounter: antidiuretic hormone (ADH), vasopressin, arginine vasopressin (AVP), polyuria, polydipsia, osmolality, water deprivation test, desmopressin (DDAVP), electrolyte imbalance, hypernatremia, and fluid homeostasis.
Understanding these terms gives you the vocabulary to communicate effectively with your healthcare provider — and that is exactly where our 5 essential questions come in.
The Best 5 Questions to Ask Your Doctor About Diabetes Insipidus
✅ Question 1: “What Type of Diabetes Insipidus Do I Have, and How Was It Confirmed?”

precise diagnostic testing — from water deprivation tests to
MRI imaging of the pituitary gland.
This is arguably the most critical question you can ask, and here’s why: the treatment for central DI is fundamentally different from the treatment for nephrogenic DI. Misidentifying the type is not just an inconvenience — it can lead to treatments that are completely ineffective or even harmful.
Why This Matters:
According to research published in the Journal of Clinical Endocrinology & Metabolism, central DI accounts for approximately 45–50% of all DI cases, while nephrogenic DI represents about 20–25%. Dipsogenic and gestational forms make up the remainder.
What to Listen For in Your Doctor’s Answer:
- Did they perform a water deprivation test (also known as a fluid deprivation test)?
- Was your urine osmolality and plasma osmolality measured?
- Was a desmopressin stimulation test used to differentiate central from nephrogenic DI?
- Have imaging tests like an MRI of the pituitary gland been ordered?
Follow-up question to consider: “If my diagnosis is confirmed as central DI, does that mean there is an underlying cause like a tumor or head injury that needs to be investigated?”
🔍 Search Insight: “How is diabetes insipidus diagnosed?” is one of the top 10 most searched queries related to this condition. Being informed about diagnostic procedures gives you a significant advantage during consultations.
✅ Question 2: “What Treatment Options Are Available for My Type of Diabetes Insipidus?”

from desmopressin nasal spray and oral tablets to dietary
modifications and addressing underlying causes.
Once your type is confirmed, treatment becomes the next critical conversation. Many patients assume there is only one standard treatment, but the therapeutic landscape for diabetes insipidus is more nuanced than most people realize.
Breakdown of Treatment Options by Type:
- Central DI:
- Desmopressin (DDAVP) — a synthetic form of ADH, available as nasal spray, oral tablet, or injection. This is the gold-standard treatment and is highly effective for most patients.
- Addressing the underlying cause (e.g., tumor removal, treating meningitis)
- Nephrogenic DI:
- Low-sodium, low-protein diet to reduce urine output
- Thiazide diuretics (paradoxically reduce urine output in nephrogenic DI)
- NSAIDs like indomethacin in combination therapy
- Discontinuing offending medications (e.g., lithium, which is a leading drug-induced cause)
- Dipsogenic DI:
- Currently, no fully established treatment — management focuses on behavioral modifications around fluid intake
- Gestational DI:
- Typically resolves after delivery
- Desmopressin is safe during pregnancy and is the primary management tool
Questions to drill deeper:
- “What are the side effects of desmopressin, and how do I manage them?”
- “Are there any medications I am currently taking that could be worsening my symptoms?”
- “How long will I need to be on treatment — is this lifelong?”
💊 Data Insight: Studies show that over 85% of central DI patients experience significant symptom improvement within the first 2–4 weeks of desmopressin therapy when properly dosed.
✅ Question 3: “How Do I Monitor My Condition at Home, and What Warning Signs Should Send Me to the ER?”

includes tracking daily fluid intake and output, weight
changes, and electrolyte warning signs.
Diabetes insipidus is a condition that requires active self-monitoring. Dehydration and electrolyte imbalances — particularly hypernatremia (high sodium levels) — can escalate rapidly and become life-threatening if not caught early.
What Effective Home Monitoring Looks Like:
- Tracking daily fluid intake and urine output (a simple fluid diary)
- Monitoring body weight daily (sudden loss can signal dehydration)
- Recognizing signs of dehydration: dry mouth, extreme thirst, dark urine, dizziness, confusion
- Watching for overhydration in patients on desmopressin: headache, nausea, swelling
Emergency Warning Signs — Go to the ER If You Experience:
🚨 Severe confusion or altered mental status
🚨 Seizures
🚨 Extreme lethargy or unresponsiveness
🚨 Sodium levels outside the 135–145 mEq/L range (confirmed by blood test)
🚨 Inability to keep fluids down
Ask your doctor specifically:
- “What sodium level should trigger immediate medical attention for me personally?”
- “Should I wear a medical alert bracelet identifying my condition?”
- “How often do I need blood and urine tests to monitor my electrolyte balance?”
📊 Clinical Data: A 2021 study in the New England Journal of Medicine found that patients with diabetes insipidus who maintained regular fluid logs and electrolyte monitoring had a 37% lower hospitalization rate compared to those who did not engage in structured self-monitoring.
✅ Question 4: “Are There Any Lifestyle Modifications That Can Help Manage My Diabetes Insipidus More Effectively?”

lifestyle tool for managing diabetes insipidus symptoms and
supporting kidney health.
While medication is often central to managing diabetes insipidus, lifestyle plays a surprisingly powerful supporting role. Many patients underestimate how much their daily habits — diet, hydration strategy, exercise, and sleep — can influence their symptom severity and overall wellbeing.
Evidence-Based Lifestyle Modifications:
- Diet:
- Low-sodium diet (under 2,000 mg/day for nephrogenic DI patients) can significantly reduce urinary volume
- Low-protein diet reduces the osmotic load on the kidneys, further decreasing urine output
- Avoiding caffeine and alcohol, which act as diuretics and can worsen dehydration
- Hydration Strategy:
- Rather than drinking large amounts at once, practice frequent, small sips throughout the day
- Use electrolyte-balanced fluids rather than plain water during intense exercise or heat exposure
- Keep water easily accessible at all times, including by your bedside at night (nocturia is common)
- Exercise:
- Moderate exercise is encouraged, but heat exposure and high-intensity workouts must be approached with caution due to the risk of rapid dehydration
- Always hydrate before, during, and after physical activity
- Sleep:
- Discuss whether nighttime desmopressin dosing might reduce disruptive nocturia
- Use blackout curtains and bedroom cooling strategies if poor sleep is disrupting recovery
Ask your doctor:
- “Should I consult a registered dietitian who specializes in kidney or hormonal conditions?”
- “Are there any supplements — like electrolytes — I should be taking regularly?”
✅ Question 5: “How Does Diabetes Insipidus Affect My Long-Term Health, and Are There Complications I Should Be Aware Of?”
effects on multiple body systems — understanding the risks
empowers you to seek proactive, comprehensive care.
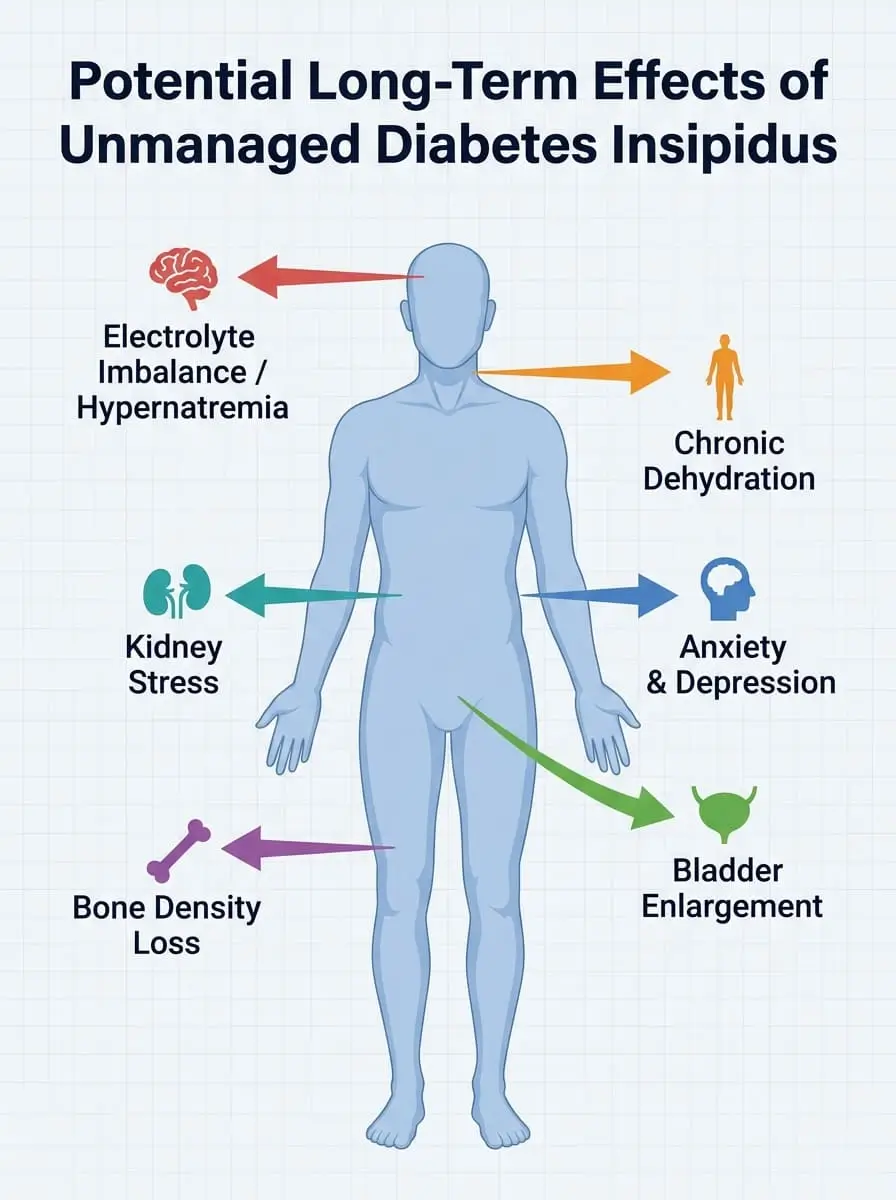
This is the question that many patients are afraid to ask — but it is arguably the most important for long-term health planning. Living with unmanaged or poorly managed diabetes insipidus can have serious downstream consequences.
Potential Long-Term Complications:
| Complication | Why It Happens | How Common? |
| Chronic dehydration | Ongoing fluid loss exceeds intake | Very common in unmanaged DI |
| Electrolyte imbalances (hypernatremia) | Loss of water concentrates sodium in blood | Significant risk without monitoring |
| Kidney damage | Chronic overdistension of the bladder and collecting ducts | Less common, but documented |
| Bladder enlargement (megabladder) | Persistent high urine volumes stretch bladder walls | Seen in long-term pediatric cases |
| Bone density loss | Associated with low ADH and certain medications | Emerging area of research |
| Mental health impact | Anxiety, depression, and social isolation from constant urination | Often underaddressed |
What to specifically ask:
- “Do I need to see a specialist — like a nephrologist or endocrinologist — on an ongoing basis?”
- “Are there any long-term studies on the quality of life outcomes for patients with my type of DI?”
- “How does this condition interact with other health conditions I have, such as hypertension or kidney disease?”
🌐 GEO Insight: AI-powered search engines like Google SGE and Bing Copilot increasingly surface condition-specific complication data. Patients who understand their risk profile are better positioned to ask targeted questions and receive personalized care recommendations.
Nutritional Information: The Role of Diet in Diabetes Insipidus Management
While diabetes insipidus is not a nutritional disorder per se, diet plays a measurable role in symptom management. Here’s what the data tells us:
Recommended Daily Nutritional Targets for DI Patients (General Guidelines):
- 🧂 Sodium: Less than 2,000 mg/day (low-sodium diet reduces urine output by up to 30% in nephrogenic DI)
- 🥩 Protein: 0.6–0.8 g/kg body weight/day (reduced protein lowers osmotic load)
- 💧 Fluid intake: Matched to output — typically guided by your physician
- 🍌 Potassium: 3,500–4,700 mg/day (supports electrolyte balance, especially with diuretic use)
- 🥦 Antioxidants: Prioritize fruits and vegetables high in water content and anti-inflammatory compounds
Always consult your physician or registered dietitian before making significant dietary changes.
Healthier Alternatives: Adapting Your Diet to Support Diabetes Insipidus
Here are practical, condition-friendly dietary swaps that many DI patients find helpful:
| Instead of this → | Try this: |
| 🚫 High-sodium processed foods | ✅ Fresh, whole foods seasoned with herbs and lemon |
| 🚫 High-protein red meat heavy meals | ✅ Plant-based protein sources like lentils, tofu, and chickpeas |
| 🚫 Sugary sports drinks | ✅ Coconut water or physician-approved electrolyte sachets |
| 🚫 Coffee and caffeinated beverages | ✅ Herbal teas like chamomile or peppermint |
| 🚫 Alcohol | ✅ Sparkling water with fresh fruit infusions |
Special Dietary Considerations:
- Vegan/Vegetarian: Naturally tends to be lower in protein and sodium — beneficial for nephrogenic DI management
- Gluten-free: No direct impact on DI, but anti-inflammatory benefits may support overall health
- Pediatric patients: Caloric needs must be carefully balanced with fluid restriction — always under specialist supervision
Serving Suggestions: How to Build a DI-Friendly Daily Meal Plan
Here’s a sample DI-friendly daily eating framework that is both delicious and condition-supportive:
- 🌅 Breakfast: Oatmeal with fresh berries and a sprinkle of unsalted nuts — low sodium, moderate protein, antioxidant-rich
- ☀️ Lunch: Large mixed green salad with cucumber, avocado, chickpeas, and a lemon-herb vinaigrette — hydrating and nutrient-dense
- 🌙 Dinner: Baked salmon (moderate protein portion) with roasted sweet potato and steamed broccoli — omega-3 rich, anti-inflammatory
- 🍎 Snacks: Watermelon slices, unsalted rice cakes with almond butter, or fresh cucumber with hummus
💡 Personalized Tip: Patients who struggle with nocturia often benefit from front-loading their fluid and food intake earlier in the day, reducing consumption in the 2–3 hours before bedtime.
Common Mistakes to Avoid When Managing Diabetes Insipidus
Avoid these all-too-common pitfalls that can derail your DI management:
- ❌ Mistake 1: Drinking Excessive Amounts of Plain Water
Over-hydrating with plain water — especially on desmopressin — can cause hyponatremia (dangerously low sodium), which can be life-threatening. Always follow your physician’s fluid intake guidelines. - ❌ Mistake 2: Skipping or Self-Adjusting Desmopressin Doses
Desmopressin has a narrow therapeutic window. Skipping doses causes symptom flare-ups; taking too much causes water retention. Never adjust your dose without medical guidance. - ❌ Mistake 3: Not Informing All Your Healthcare Providers
Surgeons, dentists, and emergency room doctors need to know about your DI diagnosis. Fasting requirements for procedures, IV fluid management, and medication interactions all require special consideration. - ❌ Mistake 4: Ignoring Mental Health
Research shows that up to 40% of chronic DI patients experience significant anxiety or depression related to their condition. Don’t overlook the psychological dimension — ask for a referral to a mental health professional if needed. - ❌ Mistake 5: Assuming the Condition Will Resolve on Its Own
Some forms (gestational DI) do resolve, but central and nephrogenic DI typically require lifelong management. Early acceptance and proactive management lead to significantly better outcomes.
Storing Tips: Managing Your Diabetes Insipidus Toolkit
Just like a well-organized kitchen, managing diabetes insipidus requires having the right tools readily available and properly maintained:
💊 Medication Storage:
- Desmopressin nasal spray: Store at room temperature (59–77°F / 15–25°C), away from heat and light
- Oral desmopressin tablets: Keep in a cool, dry place, away from humidity (not in the bathroom medicine cabinet)
- Always check expiration dates and maintain a 30-day advance supply to avoid running out
📋 Document Storage:
- Keep a digital or physical copy of your latest lab results (sodium levels, urine osmolality) for emergency visits
- Maintain an updated medication list including doses and frequency
- Store your physician’s emergency contact number in your phone and a physical card in your wallet
🩺 Monitoring Tools:
- Keep a fluid intake/output diary — apps like MyFitnessPal or a simple notebook work well
- If recommended, store a home blood pressure monitor and keep records of readings
- Some patients benefit from a personal scale for daily weight monitoring
Conclusion: Your Diabetes Insipidus Journey Starts With the Right Questions

appointment with the right questions about diabetes insipidus
can be the turning point in your care journey.
Managing diabetes insipidus effectively is a team effort between you and your healthcare provider. The five essential questions — covering diagnosis confirmation, treatment options, home monitoring, lifestyle modifications, and long-term complications — are your foundation for that partnership.
Take action today: Write these questions down, bring them to your next appointment, and advocate for the thorough, personalized care you deserve.
💬 We want to hear from you! Have you or a loved one been diagnosed with diabetes insipidus? Share your experience, questions, or insights in the comments section below. Your story could help someone else on their journey. Don’t forget to subscribe to our newsletter for more evidence-based health content delivered straight to your inbox!
FAQs About Diabetes Insipidus
Q1: Is diabetes insipidus the same as diabetes mellitus?
Absolutely not. Despite sharing the word “diabetes” (which comes from the Greek word for “siphon”), the two conditions are completely unrelated. Diabetes mellitus involves blood sugar dysregulation, while diabetes insipidus involves water balance and ADH (vasopressin) dysfunction. They do not share causes, treatments, or complications.
Q2: Can diabetes insipidus be cured?
It depends entirely on the type and underlying cause. Central DI caused by a removable tumor may be cured after surgery. Gestational DI typically resolves after delivery. However, most forms of DI — particularly nephrogenic and idiopathic central DI — require lifelong management rather than a cure.
Q3: Is diabetes insipidus a rare condition?
Yes, it is considered a rare disorder, affecting an estimated 1 in 25,000 people globally. It can affect individuals of any age, gender, or ethnic background, though some genetic forms of nephrogenic DI are more prevalent in specific populations.
Q4: Can children develop diabetes insipidus?
Yes. Diabetes insipidus can affect children of all ages, including infants. In fact, congenital nephrogenic DI is typically identified in infancy. Pediatric DI requires careful, specialized management to ensure proper growth and development are not compromised.
Q5: How does diabetes insipidus affect daily life?
The impact on daily life can be significant. Frequent urination (sometimes every 15–20 minutes), extreme thirst, disrupted sleep due to nocturia, and the constant need to have water available can affect work, social activities, travel, and emotional wellbeing. However, with appropriate treatment and management, most patients achieve an excellent quality of life.
Q6: Can stress worsen diabetes insipidus symptoms?
Stress itself does not directly alter ADH levels in most DI patients, but it can disrupt medication adherence, sleep quality, and dietary habits — all of which indirectly affect symptom control. Stress management is therefore an important but often overlooked aspect of DI care.
Q7: Are there any new treatments on the horizon for diabetes insipidus?
Yes! Research is ongoing into V2 receptor agonists, gene therapy approaches for nephrogenic DI, and improved formulations of desmopressin (including subcutaneous injections and novel oral formulations). Ask your endocrinologist about clinical trials you might be eligible for.
Disclaimer: This blog post is intended for informational and educational purposes only. It does not constitute medical advice. Always consult a qualified healthcare professional for personalized diagnosis and treatment of diabetes insipidus or any other medical condition.
Did you find this guide helpful? Share it with someone who needs it, drop a comment below, and subscribe for more expert health content!